Reproductive Health Empowerment Through Telehealth (REHEAT) Summary
New
Leveraging telehealth to support men to access credible information on modern contraception.
As low- and middle-income countries transition from paper to digital systems, family planning programs can benefit from unprecedented opportunities to improve services. Investments in digital health tools have expanded exponentially, but information on what works—and what does not— remains limited and scattered. As investments have increased, digital applications and data fragmentation have proliferated, but stakeholders are moving towards more coordinated efforts to scale digital health solutions, support countries’ digital health infrastructure, and share evidence-based learnings.
This Digital Health Compendium enables users to explore case studies across a range of digital health technologies used to enhance family planning programs mainly in sub-Saharan Africa, but also in other regions of the world. Digital health applications in family planning programs can be broadly classified as those affecting demand generation, service delivery, supply chain management, and the policy and enabling environment. In many low- and middle-income countries, digital health innovations were adopted earlier in other health sectors, including HIV/AIDS, maternal and child health, and noncommunicable disease prevention and response. As a result, much of the impact evidence is likewise restricted to those sectors. To advance greater adoption of digital technology in family planning programs, more data and information on the challenges, opportunities, scalability, and results are needed. This compendium aims to consolidate emerging information and data on applications of digital technology in family planning programs to inform adoption and scale-up of successful approaches.
All of the case studies were submitted by the implementing organizations and include a description of the digital health intervention, program context, and, if available, important findings and lessons learned through rigorous evaluations or program data. The compendium facilitates a quick search for case studies based on the target user for digital health intervention, building block for the digital health enabling environment, family planning program classification, and country location. The case studies give policy and program decisionmakers insights on real-world applications of digital health, promising practices, challenges, and other lessons that can be applied to current and future programs.
New
Leveraging telehealth to support men to access credible information on modern contraception.
Dr. John Mark Bwanika
Director Operations, Research and Projects
Email
The Medical Concierge Group(TMCG)
Ongoing
The Medical Concierge Group(TMCG): Designed and deployed the telehealth platforms leveraged during project implementation.
The National Academies of Sciences, Engineering, and Medicine under the Partnership for Enhanced Engagement in Research (PEER) funding mechanism.
Kampala, Uganda
Client
Services and Applications
Demand Generation
African population growth is extremely rapid, with all countries growing at annual rates of over 3%.[1] Uganda’s population averages 46 million people, representing about 30% growth from 36.9 million per the last national population census in 2014. [2] Uganda’s total fertility rate is 6.2 and the median age at first sexual intercourse is 16.8 years, an age considered to be vulnerable to sexual and reproductive health (SRH) challenges. [3] The uptake of modern contraception in Uganda has remained suboptimal at 30% (contraceptive prevalence rate), with the current unmet need for family planning among women placed at 34%. [4, 5] Men make most decisions at home, but unfortunately, their involvement in SRH issues has always been very low. Promoting male involvement in family planning is an excellent approach to decreasing the unmet need.
Several factors have been identified to account for the above trends including lack of access to credible information on modern contraception, lack of male partner support/engagement in decision making, poor or nonfunctional post-service follow-up mechanisms to address challenges like side effects, myths, and misconceptions among others. [6, 7] The REHEAT project aimed to assess the feasibility, acceptability, and impact of the Men’s Telehealth Information Package (mTIP) on uptake of family planning and reproductive health services among their spouses.
The primary target audience was sexually active Ugandan men aged 18-55 years, having a spouse or current sexual partner with access to a mobile phone, and willing to participate in all study-related activities. The secondary audience was the spouses of the men who participated and had to be aged between 18-55 years.
Recruitment took place at community settings such as sports events, village council meetings, religious gatherings, and university premises. In addition, social media and other digital platforms were leveraged to share information about the study.
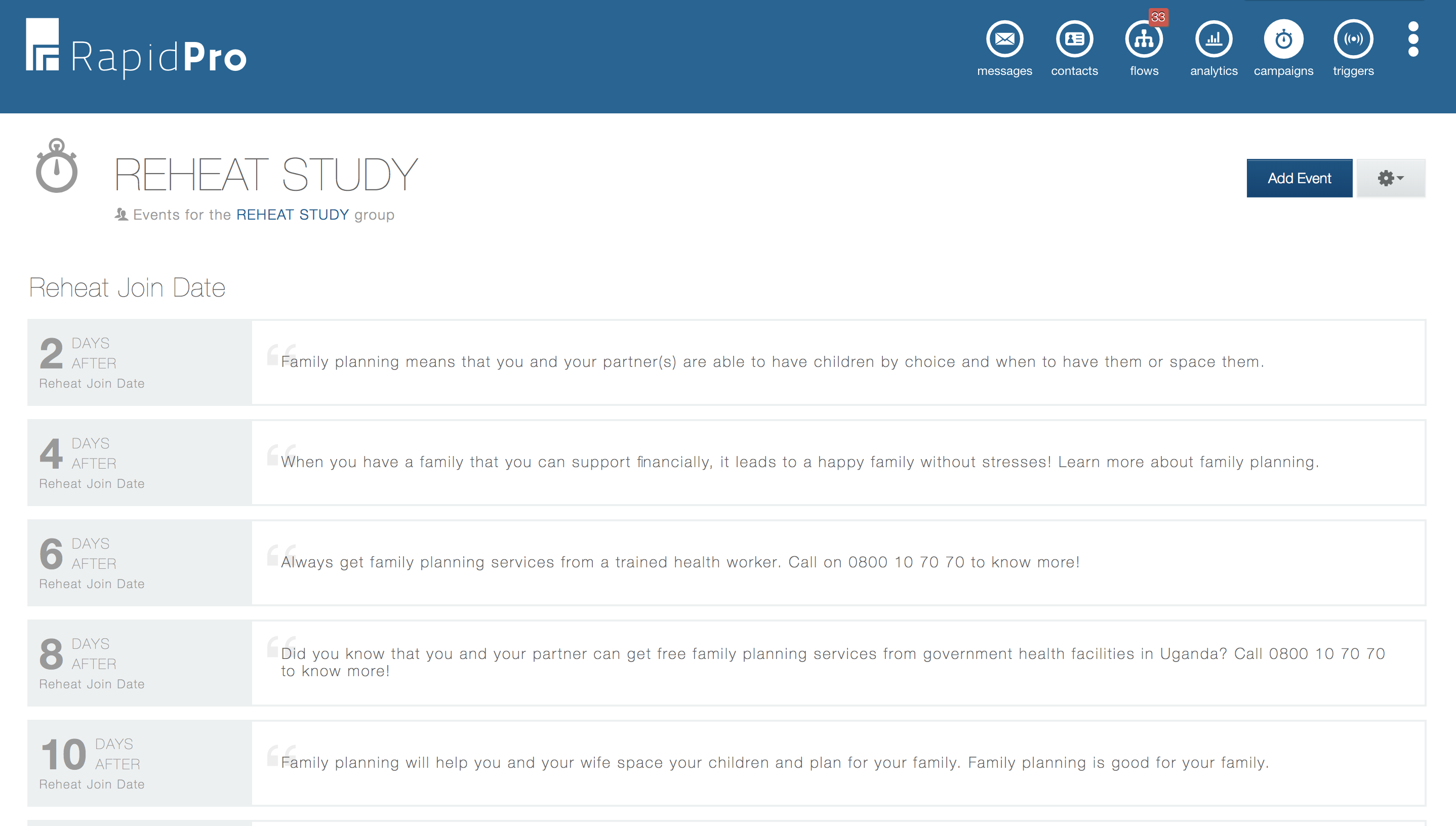
Eligible participants who consented to participate in this pilot study were asked to send a trigger word ‘RH’ to a prepaid study SMS shortcode to access mobile health messages on family planning. The mobile messages covered aspects of informational, motivational, and behavioral aspects of modern contraception intending to cause behavioral change towards stimulating conversation with spouses on family planning and eventual uptake. The content was translated and made available in both English and Luganda (a local language).
In addition, the men had access to qualified health professionals for remote resolution of inquiries via teleconsultation on a toll-free hotline (0800 107070). This hotline was available 24/7 and operated through a medical call center. The men were followed up over 6 months with periodic voice call follow-ups at months 1, 4, and 6 from enrollment to assess family planning knowledge acquisition, partner conversation on modern contraception, and possible uptake.
A total of 551 participants (450 males and 101 spouses) were onboarded onto the study and followed up for 6 months. By the end of the six months, 432 males and 97 females were still onboard.
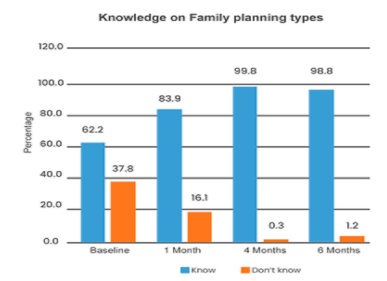
A total of 26,988 mobile short messages (SMS) were sent out over the six months. An average of 66 messages were received by each study participant. Out of the 450 males onboarded on the family planning mobile messages, 426 (95%) successfully received the messages, and only 24 reported not having received the mobile health content. In addition, the average response rate to the weekly quizzes was 23% for periodic quizzes. Thus, there was a 58% increase in high knowledge of family planning in 6 months
After 6 months, there was an 18% increase in family planning uptake and this was attributed to the improvement in communications on its uptake amongst spouses due to men having received mTIP. 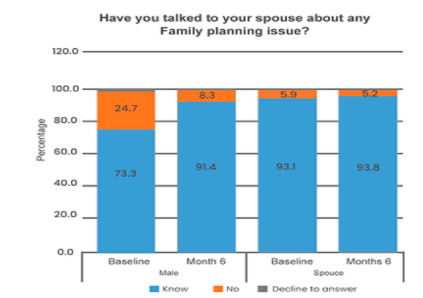
After completion of the six months, some study participants quoted:
“This study has enabled us…to come together as partners. You know in our local setting, we don’t want to share this…with our wives…it has enabled us to realign our education about family planning…”
“She used to hide it from me…Then when this study came in, she told me about Depo, then I said it would be better if you go in for that…”
i. Male engagement
Mobile phone-based channels of health information exchange can reach men that are often left out in the traditional health facility-based and media communication channels. In addition, educating men as agents to champion the use of family planning to partners helps promote faster uptake of the services since these men are currently dominant decision-makers at home.
ii. Accessibility
The two-way communication channels (i.e. toll-free hotline and SMS platforms) used in the REHEAT pilot offered easy access to credible family planning information. In addition, the immediate response to the client’s concerns encourages continuous engagement and use of mHealth interventions among target beneficiaries.
iii. Scalability
Over 26,988 messages disseminated without any physical interface using mobile platforms show the potential impact and reach of digital approaches in information dissemination at a large scale.
iv. Operationality
Continuous monitoring of the performance and functionality of digital platforms is key in achieving the expected intervention objectives. As noted, downtimes and message sending failures were among the challenges the REHEAT pilot faced.
Digitally supported communications channels for health information dissemination on family planning allow for a wider reach with minimal resource input regarding contact time and space yet allow for customization to specific demographics. In addition, availing channels to address beneficiaries’ concerns and inquiries in real-time or as fast as possible helps to increase the likelihood of the adoption of family planning among couples. Our next step is to scale up the REHEAT project to cover the entire Kampala city to test the package’s scalability and sustainability models.