INTRODUCTION
Uganda’s mobile phone penetration stands at 60.3% [28.01 million] with about 13 million people using smartphones. [1] Many digital solutions have been built to support smartphone users, leaving out users with feature phones who are part of the significant percentage of mobile users in Uganda, standing at 15 million. In order to make informed decisions, people need to access accurate, reliable, and timely information and services, and this has been a challenge for many. Given this, Reach A Hand Uganda developed the USSD to create a linkage to services and information by simply dialing *284*15# on your mobile phone.
ABOUT SAUTIPLUS
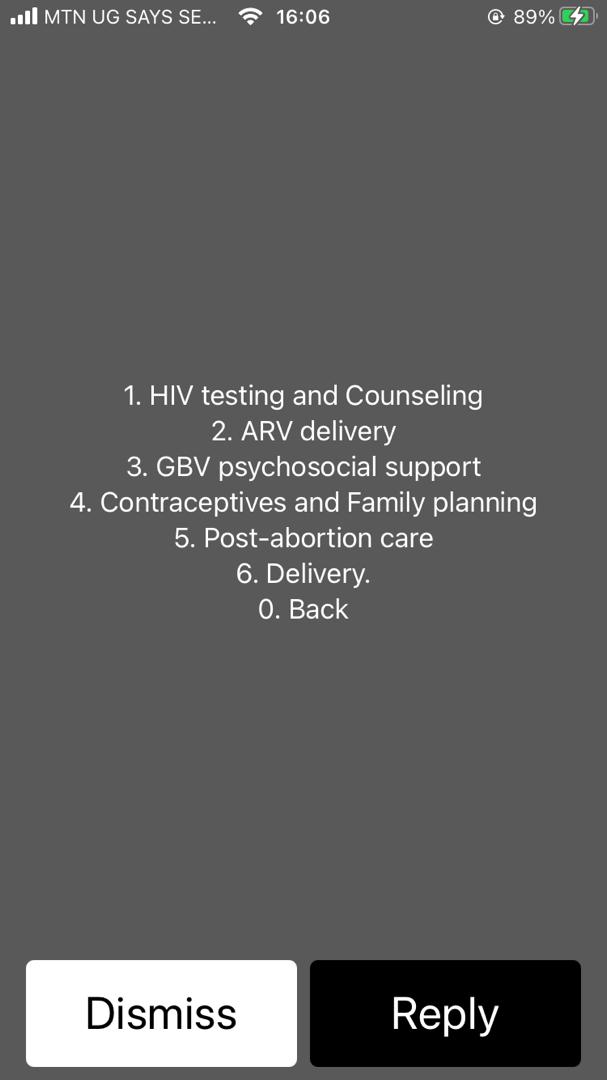
The SAUTIplus USSD is an innovation by Reach A Hand Uganda to increase referral and linkages of users to the nearest health facilities to get services and also through subscriptions, the users can
get notifications on both tailored or general SRH information. The USSD code enables cellular telephones to communicate with the mobile network operator’s computers to seek sequential data or information as per the caller’s needs. Services for referral linkage range from HIV testing and counseling, Antiretroviral (ARV) delivery, Gender-Based Violence (GBV) and psychosocial support, contraceptives and family planning, post-abortion care, and delivery.
By simply dialing *284*15#, open to all local networks at no cost, the users can request information and any referral and linkage to clinics, hospitals, and health facilities that offer family planning and contraception in a discrete way. Users receive a text message on the closest clinic, times when it’s open, the contact person and in case there is a need for counseling before visiting the clinic, in the message we ensure to add a toll-free line to call for better guidance and counseling or encouragement to visit the health facility.
EVALUATION AND RESULTS
A performance evaluation was implemented through a desk review with a dataset extracted from
May to September 2020. The evaluation was based on the utilization of the USSD amongst the
young people ages, 10-24.
A total of 1297 requests were made from May to September. 
Age and services requested.
The age group 15-19 and 20-24 which we target with our services mainly sought HIV testing, counseling, contraceptives, family planning from May to September 2020.
An analysis of the calls and SMS messages during this time period indicates that youth experience
unsafe sex during this period, and a lack of accurate information on where to get the services. This was especially prevalent in June when 41 clients requested contraceptives and family planning and 49 requested HIV testing and Counseling.
Age group 25 and above

The age group 25 and above mainly sought out GBV psychosocial support, HIV testing and
counseling, contraceptives, and family planning. The USSD was circulated during the time when the COVID-19 lockdown had just been lifted, though, with stringent measures still in place, many people found difficulties with transportation and also had the fear of contracting COVID-19 from the health facilities. This age group mainly consists of people who are married or living with a partner hence the high demand for the above-stated services.
To achieve the desired health outcome, a system evaluation was carried out to ensure that health
information is well aligned with the referral aspect to complete the cycle. It triggered a system integration effort which included the development of new content (e.g., health information per thematic area and health facilities) with a clear direction of what particular services one requires for linkages, such as a direct request for HIV test or HIV counseling or medication with an extension for delivery.
LESSONS LEARNED
There is a need for integration with all health facilities country-wide with support from MOH. The data shows that there hasn’t been a comprehensive mapping of all health facilities countrywide
including private, government, and any other (e.g., church and Non-Governmental Organizations NGOs). This comes as a concern that people may be deprived of basic referrals due to many not offering certain services on the service list of the USSD.
There is a need for Integration with a call center to offer a 360-degree service control of follow-ups and inquiries.
CONCLUSION
The SAUTIplus USSD has been a revolutionary innovation with over 150,000 dialers, over 5,000 subscribers, and over 6,000 successful referral and linkages in the space of 15 months. There are opportunities for more improvements in design focusing on human-centered design [HCD] principles to reach last-mile users. We intend to reach out to more people in the country to continually improve reproductive, maternal, newborn, child, and adolescent health outcomes countrywide.
REFERENCES/RESOURCES
- DATAREPORTAL (2021) Digital 2021: Uganda. https://datareportal.com/reports/digital-2021-uganda
- https://africastalking.com/ website [Last accessed on December 4th, 2021]